
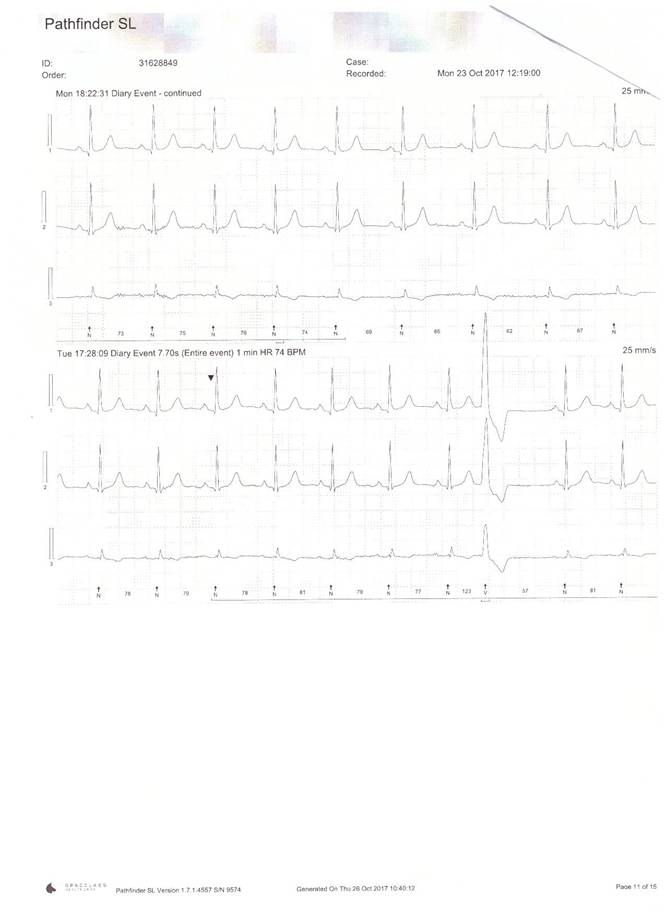
Ambulatory heart recorder trace of a patient suffering with ‘skipped beats’. Note ‘large’ beat on bottom of trace (8th beat along) is a ventricular ectopic beat or PVC

Ambulatory heart recorder trace of a patient suffering with ‘skipped beats’. Note ‘large’ beat on bottom of trace (8th beat along) is a ventricular ectopic beat or PVC